For the elements whose value is from a set of (coded) options, a FHIR ValueSet should exist. SMART Guidelines can use Common ValueSets or define new ones.
ValueSets are used in
Logical Models
Profiles
Questionnaires
The L3 should use same codes as defined for LM
TO DO: Do we add a codesystem also for the discrete values e.g. male, female, etc
Inputs:
DAK
SMART IG ValueSet catalog
Terminology services to lookup and validate the codes
Outputs:
ValueSets in input/valuesets or input/fsh/valusets
Proposal for any common value sets
If a valueset changes since the last release, see tracking changes.
Valueset usage registry?
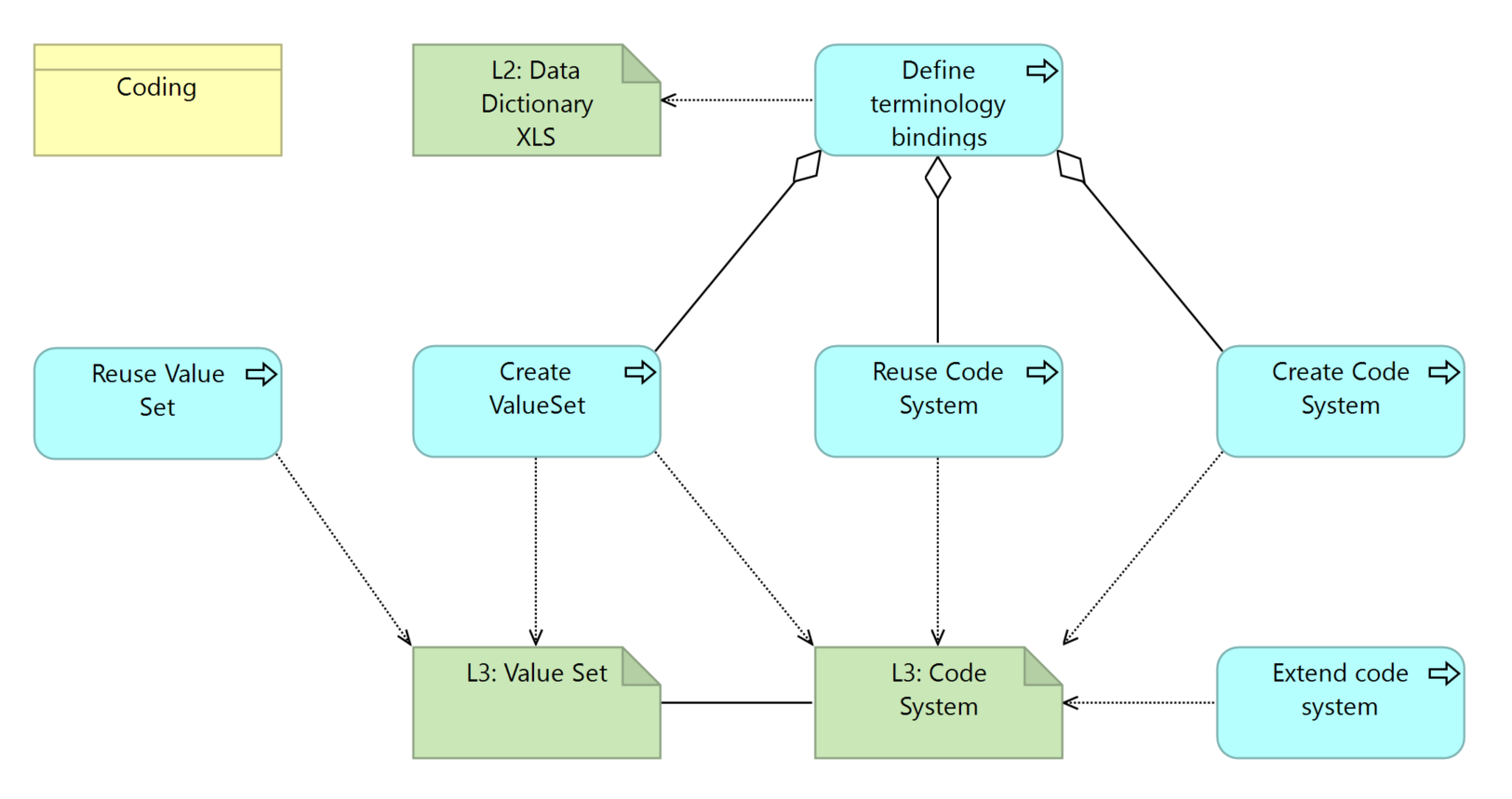
Activities:
This is the overview of the activities and related artifacts used:
For each element in the DAK that has a value set - i.e. the answer depends on the options for the data element - for example sex, etc., the author shall have a value set. this can mean
reusing a value set
TO DO: Common Value Sets repository
Creating a new value set
only for the purpose of the current SMART Guideline
as a candidate for common value set
functionally, the valueset in the L3 level must support the L2 expressed values.
However, the actual codes are typically a L3 decision, unless the L2 imposes some codes.
preferred:
ICD-11
LOINC
ICD-(others)
Open and globally available code systems without licensing restrictions
Jurisdictionally endorsed or required codes
Note that FHIR has codes that may be required or extensible - in these cases the FHIR values should be preferred - however, concept maps SHALL be in place between these codes and the codes above.
NOT The DE.5.1 whatever codes
TO DO: How to decide?
TO DO: Does the VS in the LM match the VS in the profiles? Why would it? FHIR VS may change, and we don't want that.
The creation of a value set may require the creation of a new code system
start
The creation of a value set may, in some cases, require changes to the profiles: If a FHIR resource has a binding that is too strict and the L2 model requires a broader value set, normally a new element or extension must be created.
For example, adding a gender “changed” to the Administrative Gender Value Set - that is not supported and would require mapping the element and its value set to a new extension in FHIR.
Given the impact of this, any such deviations should be identified and discussed with the L2 author who can evaluate consistency, value, and the real need.
TO DO: Decision tree.. including profile, and proposing to ICD-11 governance entity.
ValueSet creation:
Add “Shareable”, “publishable” extensions
ValueSet reutilization:
ValueSets may be reused if the application needs are consistent.
While reusing of ValueSets is recommended, authors should be aware that a reuse also introduces a dependency
ValueSet validation: The ValueSet should be valid against the SMARTValueSet profile
CodeSystem creation
When defining a ValueSet, there may be a perceived need to create a CodeSystem:
TO DO: When do we create a code system? When do we select codes from an existing code systems
Review procedure
ValueSets shall be reviewed for criteria
Output Criteria / Definition of Done:
All the elements in the L3 that have coded values shall have a corresponding valueset
All the values in the valueset shall be valid codes:
Available in an available code set (for example no SNOMED unless SNOMED is supported)
Not deprecated
Terminology Services
lookup
mapping
validate
Change tracking
Tooling
Tool
Usage
Doc
Sushi
OCL
tx.fhir.org
Informative examples
Known issues and dependencies
TO DO: Preferred Terminology Server
Is there a relationship before ANC.B5.DE50 and the valueset name? Would the valueset for the values for that element have a similar name?
This will actually result in changes to profiles - e.g. needing a value when the existing binding is Required
TO DO: Bring out requirements for OCL as a reference terminology server - what operations, what content...